Health systems are under a variety of well-documented performance pressures, from payors, employers, individuals, vendors, and regulators. In our experience, the employed medical group is both a source of concern and an opportunity in many systems. “If only we could have our physicians do ‘X,’ it would drive significant value” has long been a common lament FORVIS has heard in our work with health system leadership. The purpose of this article is to connect some dots within recent regulatory changes permitting “value-based” compensation and broader physician alignment objectives (“value-based arrangement” or VBA), with the goal being a better understanding if the “X” your system would like to achieve can be accomplished in the near term.
The Basic Idea – Triple-Aim Pay to Providers for Triple-Aim Value
If “X” from above fits into a classic “triple-aim” framework (improving patient experience, improving the health of the population, and reducing the cost of care), then a VBA is a valuable option for a variety of common strategic and operational challenges.
Examples of Problems That a VBA Can Help Solve
The following items are common sources of frustration.
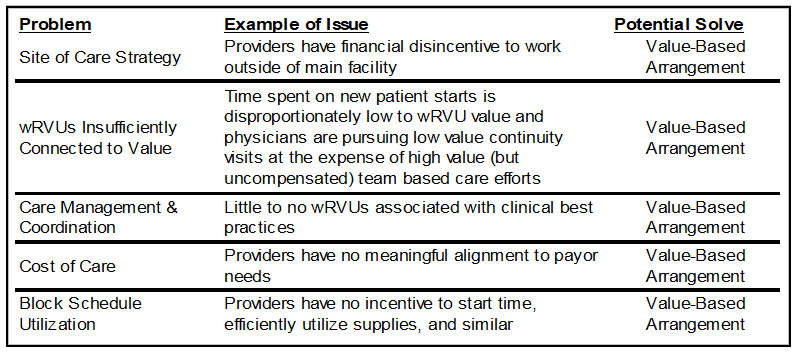
What they all really reflect are areas that conflict with value-based incentives in prevailing compensation structures. These gaps historically have been driven by the regulatory environment and Congress’ demand that providers not be financially rewarded for referrals made for certain services (“designated health services”).
CMS wants all Medicare beneficiaries to be in a care relationship with accountability for quality and total cost of care (a value-based relationship) by 2030 (Strategic Direction | CMS Innovation Center). To support this and similar objectives and to address transitioning concerns from stakeholders, in 2018, the U.S. Department of Health and Human Services (HHS) initiated its “Regulatory Sprint to Coordinated Care.” CMS has responded by granting new regulatory flexibility related to the Stark Law effective in early 2021.
In Case You Missed It – New Stark Law Exceptions
On December 2, 2020, CMS published its final rule, Modernizing and Clarifying the Physician Self-Referral Regulations (commonly called the Stark Law), which generally took effect January 19, 2021. It is outside of the scope of this article to summarize its contents, but it generally created three new “value-based” exceptions to the Stark Law.
New Physician Alignment Tool to Incentivize Value-Based Performance
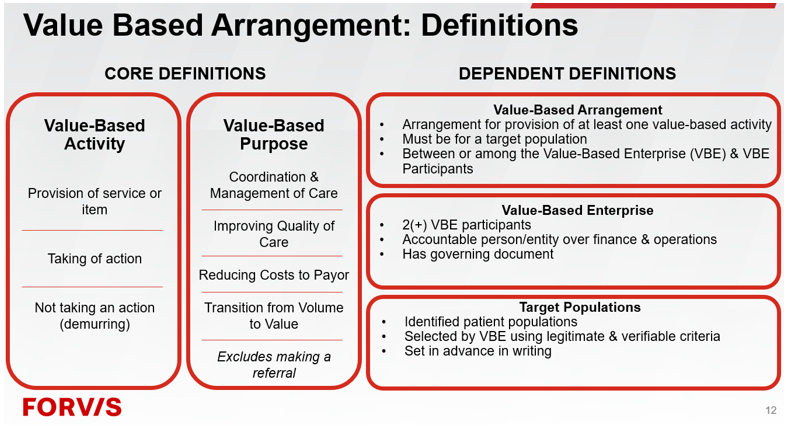
The three new Stark Law exceptions essentially represent a sliding scale of flexibility tied to financial risk and compliance burden. As there is more financial risk that is in play, there are fewer compliance requirements to adhere to with the respective exceptions. This article will generally assume organizations will utilize the Stark Meaningful Downside Financial Risk to physician(s) exception. This exception is available to arrangements where a physician has a meaningful downside financial risk (at least 10% of remuneration) for failure to achieve set in advance cost, quality, or other performance benchmarks. See Appendix A for a summary of the definitions.
It is common for employed providers to already have 5% to 15% of pay tied to various quality, patient experience, and citizenship metrics. Therefore, having 10% of remuneration converted to pay under a VBA should not itself be a significant burden. The details will matter to the provider, but the financial risk should be in a relative zone to current state for most providers.
Too Good to Be True? No! But the Arrangement Must Complement Operations
The challenge is not whether the regulatory flexibility can really address these and other hard-to-solve challenges under the historical Stark Law framework—the CMS updates to the Stark Law deliver the goods. The question really becomes whether an organization is ready to operationalize a value-based structure.
What Does “Value-Based Operations” Mean?
We believe value-based operations is an intentional design in operations around achieving triple-aim outcomes. It means incorporating data and designing clinical care protocols and community-level programs around the best fit for patients, providers, employers, and facilities in a way that fits the organization’s mission, vision, values, and strategy. This is both easy (the “what” and the “why”) and hard (the “how”). Most of the “hard” comes from creating a baseline and resetting operations to incorporate value-based objectives. Our observation is that this type of change is more about realignment than creating something new. For instance, “quality” is generally already a function that primarily interfaces with clinical operations. In a value-based framework, quality is foundational and becomes a quasi-compliance function because, if the operations team is leading falling quality, regulatory risk can appear under the new Stark Law exception if ignored for an extended period of time.
How Does One Begin Value-Based Operations & Paying Providers Under a Value-Based Exception?
Step 1 – Identify & Assess a Service Line(s)
At heart, VBAs are about professionally organized and administered, physician-led continuous performance improvement operations. Not every area in an organization will be ready for value-based operations. However, some will be more ready than others. We recommend identifying a pilot clinical area to begin the journey to value-based operations.
The assessment process is about an integrated leadership team identifying the potential for positive change from a patient, financial, and leadership perspective. In essence, it is the attempt to define to what extent there are performance improvement opportunities that fit a triple-aim framework.
Step 2 – Develop a Performance Excellence Project Plan
This second step focuses on elevating an assessed opportunity into a workflow process. This phase will include change considerations, resource requirements, reporting and accountability, budgeting, and stakeholder input and socialization. There should be enough detail to document what would change and why under a value-based operations approach.
Step 3 – Assess Performance Excellence Plan for VBA Fit for Quality
Patient quality and outcomes are central to a VBA. Establishing objectives and goals that can be managed, measured, and benchmarked is critical to a sustainable and compliant VBA. Although legal counsel should be involved throughout, this is an especially important time to receive guidance from counsel regarding whether the contemplated program principles are acceptable and all required elements and/or best practices are considered.
Step 4 – Provider Pay Design
Pay design that fits the providers’ span of control coupled with broader responsibilities that are within their span of influence is critical to operationalizing a VBA. As mentioned above, provider leadership should be focused on performance improvement activities along with the traditional needs of serving patients. This elevated form of alignment is a natural fit for what providers find most important in care delivery. There will need to be meaningful provider education, data transparency, and a deliberate change management process, but the concept of paying for high quality and efficiency rather than paying based on a wRVU will frequently resonate.
Step 5 – Operationalize & Recalibrate
New workflows, scheduling updates, collaboration and care coordination activities, coverage terms, and outcomes reporting are all examples of things that may need to change to meet the goals of a VBA. These changes will not all work perfectly on day one; instead, focus on processes that will create feedback loops to identify performance challenges and for parties to expect to make tactical tweaks on a routine basis until normalcy is established. From there, recalibration will follow a more formal business plan, budgeting, or other routine cycle.
Conclusion
Value-based operations can be a strategic pathway to elevate physician alignment, be responsive to changing goals and needs of CMS and other payors, and drive systemwide performance improvement. Day-to-day value-based operations need to be professionally administered and physician-led, similar to many existing dyad structures, but with an increased focus on triple-aim objectives. The result is patient-centric with continuous quality and cost improvement along with other benefits similar to co-management arrangements. Implementing value-based operations also requires real change around the acquisition and use of data, allocation and deployment of resources, and organizational prioritization of “value.” These changes are manageable and, with careful planning, can be made palatable to all stakeholders through a structured, multiyear transition.
Reach out to your professional at FORVIS or submit the Contact Us form below if you have questions.
Appendix A